


The Role of Medicaid Waiver Transformation Projects in Transforming the Core Strategic and business planning framework of health care organizations

 Overview
Overview
Across the United States over the last 10 years, 1115 Medicaid Waiver projects — initially known as Delivery System Reform Incentive Payments (DSRIP) projects — are driving health care transformation on a large scale in California, Texas and New York with other states such as Washington preparing to launch. These waiver-funded projects represent an unprecedented targeted investment in the statewide and local-level health care delivery system by funding projects to improve the quality of care, while lowering costs and increasing patient satisfaction. The waiver projects allow providers to receive financial payments for achievement of predefined metrics and outcomes that incentivize increased collaboration among the care coordination networks that are being established in local geographies.
New York is leveraging DSRIP to significantly restructure its health care delivery system and develop networks that can take financial risk and are incentivized to proactively engage with members to enhance wellness. The state has a primary statewide goal of reducing avoidable hospital use by 25% over five years. Up to $8 billion are allocated to ensure this program succeeds, with payouts based upon achieving predefined goals in system transformation, clinical management and population health. These funds are comprised of planning grants, provider incentive payments, and coverage for administrative costs. Another bucket of funding is set aside for other Medicaid redesign purposes to support health home development, investments in long-term care, workforce and behavioral health.
The NY DSRIP program aims to achieve the following goals:
- Safety-net system transformation at both the system and state level
- Accountability for reducing avoidable hospital use and improvements in other health and public health measures at both the system and state level
- Long-term sustainability of delivery system transformation through leveraging managed care payment reform.
In New York, DSRIP funds are funneled through 25 Performing Provider Systems (PPS) that have been chartered by the state to create care coordination and delivery networks including clinical providers and community-based organizations (CBO) across their geographies. Other states with DSRIP programs have set up or are contemplating similar structures. The PPS acts in a fiduciary role along with controls setup by the state and monitors and administrates the funds to the participating providers in the PPS network through a variety of administrative governance structures.
Background
DSRIP has triggered or accelerated changes to the core strategic and business planning framework for many healthcare organizations in New York and has the potential to change the relationships between providers, CBOs and health plans as the transition to value-based payment (VBP) takes hold. Organizational financial planning processes are one area where a critical shift is taking place. Traditional health care providers and CBOs historically not engaged in “health care” are facing major transitions due to reimbursement shifts that are pushing more risk down to the provider level. The financial incentives in early DSRIP contracts are targeting substantial modifications to the health care delivery system in how care and eventually proactive wellness and preventive services are ultimately provided to the patient.
Under DSRIP, starting in the second year and increasing over time, a greater and greater part of the dollar is tied not to process but directly to the impact on community-level health care outcomes such as reduction in avoidable ED use, inpatient admissions and impact on hypertension. These metrics also (over time) drive providers’ Medicaid managed care contracts and thus the DSRIP contracts serve as a bridge to value-based contracting for Medicaid, as well as other lines of business.
In order to succeed in drawing down the DSRIP dollars, providers are investing, individually and in groups, in the development of population health management support services. Traditional provider networks are being redefined as “partner” networks that include not just health care providers but community organizations and other social support services that can be integrated into wellness networks to achieve the Triple Aim by impacting the underlying social determinants that drive cost and patient behavior. Capital spending on facilities and information-technology are changing rapidly with some parts of the state converting hospitals into “medical villages” with an array of ambulatory and long-term services replacing inpatient beds no longer needed as care is better managed in other lower acuity settings. All of this is leading to shifts in the composition of the workforce, such as hospital employees preparing for new roles as care navigators. To fully benefit from the opportunities that DSRIP presents, organizations must give thoughtful consideration to each of these areas.
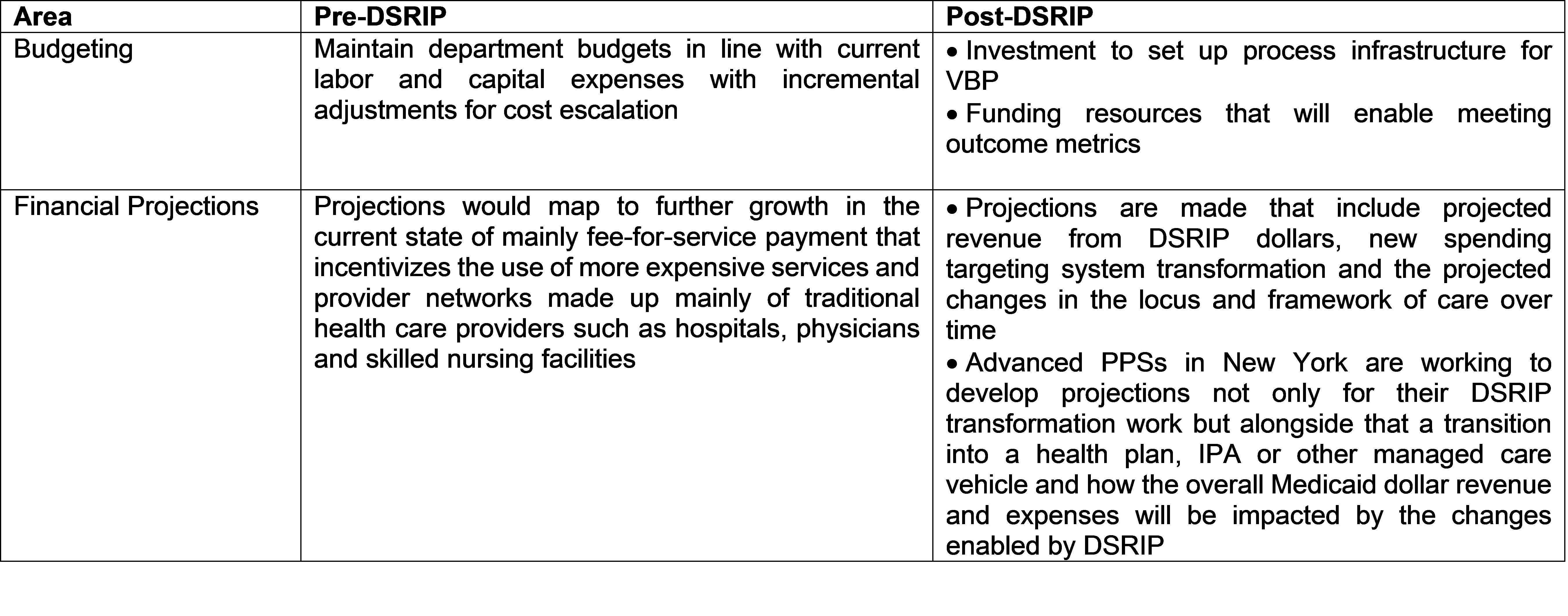
Financial Planning
There have been shifts in the financial planning processes due to the distribution of financial incentives to establish the infrastructure necessary to facilitate the transition to value-based payments. PPS leads must design the flow of state funds to the network partners as incentive payments that are released over a period of five years. Some of the larger PPS networks have several hundred partners who may be eligible for a share of the funding pool. Payment structures are designed where every eligible dollar that a partner can draw down from the PPS is at risk and is tied to meeting prescribed milestones and metrics. Over time the dollars become more at risk as the payments become more outcome-based, further placing the providers on the readiness trajectory towards VBP arrangements both operationally and culturally/strategically.
Workflow Transformation
There are other major healthcare delivery system changes as well that are part of the DSRIP program. In New York, system design changes to address required transformation are being addressed initially through the establishment of multiple project workgroups. These workgroups provide unique forums for stakeholders and subject matter experts from a wide array of health care service areas to come together to design, build, and implement clinical workflows to address specific gaps found in their community needs assessments. As these committees are formed and evolve, this leads to further alignment of care delivery processes between providers who have traditionally not worked together in this capacity. As a result, the right type of provider is engaged in the appropriate step of the care delivery process in the future state.For example, the objective of the Emergency Department (ED) Care Triage workgroup is to design a process to ensure patients discharged from the hospital do not rebound back to the ED by providing care coordination and management, discharge planning and, if necessary, a warm handoff with CBOs.Specific roles for non-traditional providers and organizations such as behavioral health therapists or community-based care navigators are uniquely defined in process maps with clear swim-lanes that define where handoffs and transitions will occur in future state workflows. The goal will be to enable new proactive health and wellness networks to address both health care needs as well as to impact root cause social determinants of care.

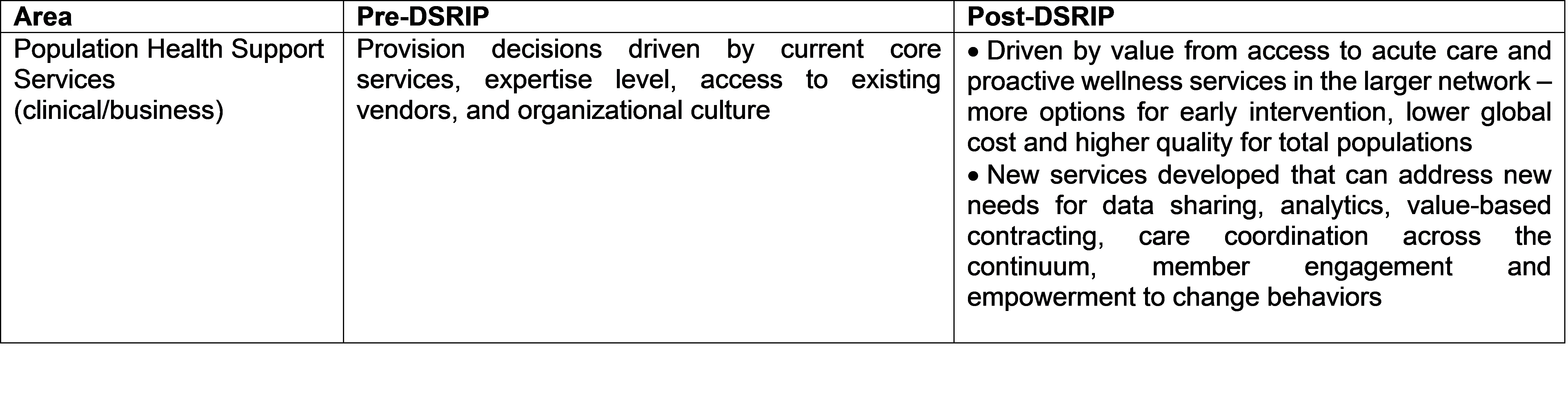
Population Health Management Support Services
DSRIP will also disrupt the provision of population health management and centralized clinical support services for providers and partners in the PPS, as well as any existing or developing IPAs or health plans. Traditionally many buy vs. build decisions on services related to care management, call center and clinical technology are made with an individual organization mindset. As the collaboration amongst multiple partners is amplified by DSRIP, a more judicious decision criteria will be developed for centralizing these services as cost efficiency from scale and prior experience/expertise is introduced.
To date hospitals, health systems and other providers have not been financially incentivized to build true population health management support systems that address the care and wellness needs of patients and members outside of traditional care sites. PPSs and their IPA and health plan future state partners will be inclined to build centralized services that can scale their services across deep networks that include not only all of the traditional health care providers in the network but also to community support organizations in an effort to reduce global costs, improve global quality outcomes for their assigned population, ensuring access to the right acuity of care and proactive wellness services at the right place at the right time and at the right cost.
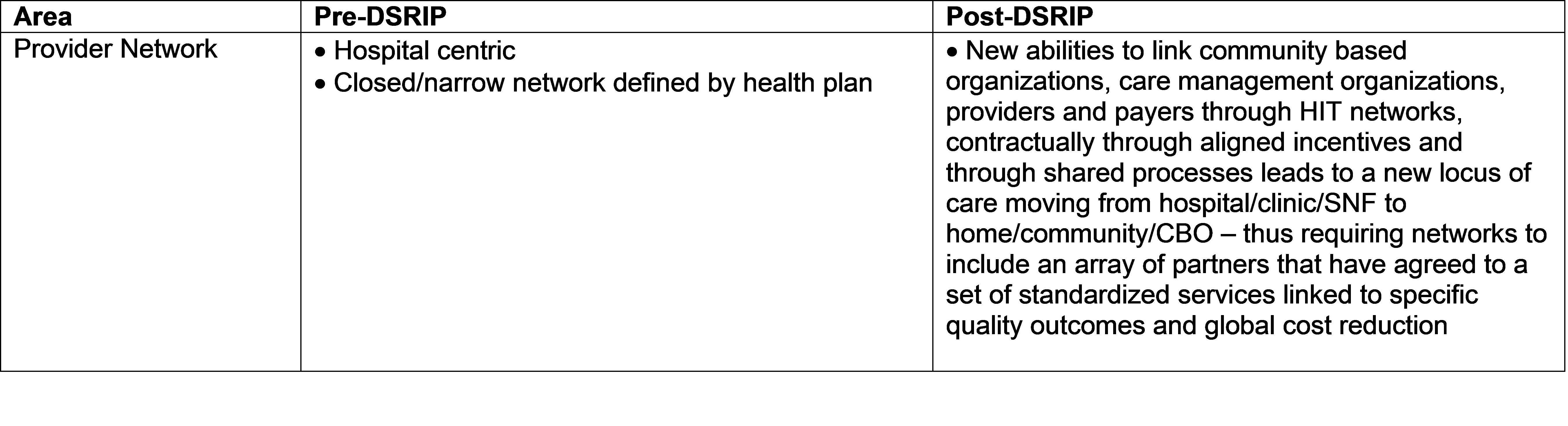
Partner/Provider Network Refinement
A final area that will be impacted is the refinement of provider networks. DSRIP created the Performing Provider Systems based on their geography with each PPS having a unique number of attributed members. Network refinement will be a naturally occurring phenomena as the selection of the right network of care vs. operating independently becomes a critical decision point. There will be a vital need to ensure there is clear mission alignment and appropriate support of the network for the provider’s success as well as infrastructure development to survive in a risk-based environment. Today’s market is dominated by large health systems all of which seek ways to reduce operating costs in the upcoming world of value-based care. An organization with low performance scores and inefficiencies (e.g. paper medical record system) will not be attractive to a provider system they are looking to join or even health plans in their negotiations if they don’t work through defining the value of their service to the community in a quantitative manner. In addition, as the delivery of care migrates to other lower acuity settings, the partner network model will shift to an emphasis on transitions of care and inclusion of CBOs.
About COPE Health Solutions
COPE Health Solutions has extensive experience in 1115 Medicaid Waivers and DSRIP, from planning stages to implementation of projects and development of successful contracting and funds flow strategies. We can assist your organization develop a successful DSRIP strategy to ensure success and integration with the changes to the VBP environment. Our team is well positioned to assist your organization develop and implement best practices in managed care, population health management, Medicaid redesign and Medicaid waivers.
For more information about how COPE Health Solutions is helping clients across the country develop and execute successful contracting and funds flow strategies that align with the shift to VBP contracts, please contact: dsrip@copehealthsolutions.com.