


 Background Information
Background Information
Basic concepts of value-based payments
As the healthcare industry continues to implement many aspects of the Accountable Care Act (ACA), much of the focus is on payment reform. One of the most commonly utilized terms about payment reform is value-based payments (VBP). As an umbrella term, VBPs can cover a wide range of payment mechanisms that are being employed by government payers and health plans nationwide. Just as we say healthcare is local, we also can say that payment mechanisms are local. Different regions of the country are experimenting with varied payment reforms, most of which have a value-based component.
Those individuals who work in the healthcare industry may already be familiar with common performance incentive payments, such as pay for performance (P4P), which is a value-based payment modifier to standard fee-for-service (FFS) payments. This specific mechanism rewards providers who meet or exceed predetermined performance metrics. California was one of the first states to develop this widely adopted payment mechanism, and many health plans in other states have followed suit.
More recently, VBP refers to advanced payment models where some level of financial risk is attributed to the provider, network of providers or other arrangement of integrated delivery networks (IDN). There are several different types of integrated delivery networks that include: clinically integrated networks (CIN), independent physician associations (IPA), integrated delivery systems (IDS), performing provider systems (PPS) and many others. The details of these partial or shared risk arrangements will be described later in this article.
How VBP relates to NY DSRIP work
In the summer of 2015, the Centers for Medicare and Medicaid Services (CMS) approved the New York State Department of Health (NYSDOH) Value Based Payment Roadmap. This document outlines the plan for VBP arrangements with government programs in New York. Very quickly, VBP became a frequent topic of discussion statewide, and the specific payment mechanisms qualifying for a degree of “value base” in NY were finally fully defined. The Medicaid program in NY was already beginning a massive 5-year transformation, fueled by the 1115 Waiver and the associated Delivery System Reform Incentive Program (DSRIP). One of the central themes of sustainable delivery system transformation is the successful and widespread adoption of VBP between the delivery system and the managed care organizations (“MCOs”) administering managed Medicaid in the state.
IDSs of Medicaid providers who are participating in New York State DSRIP are organized into Performing Provider Systems that have the responsibility of tying care delivery transformation to VBP within their service areas. The theme of DSRIP is partnership; thus, MCOs will be partnering with PPSs statewide in the coming months to develop regional work plans to reach value-based payments.
Value Based Payment Levels (as described by VBP State Roadmap)
Types of VBP
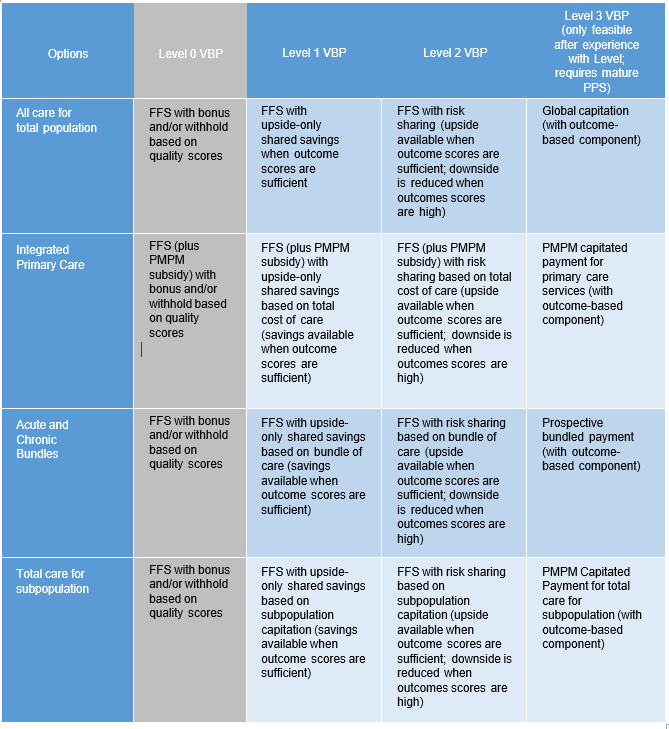
As defined in the State’s Value Based Payment Road Map, the various payment methodologies have been categorized into one of four levels. The different levels in the roadmap correspond directly to the level of risk that the organization bears. The options are organized into four categories:
- All Care for Total Population (also known as “Total Cost of Care” arrangements): These payment mechanisms take into account the total cost of all care being delivered across the full continuum. The intent is for the cost of care to be reduced year-over-year. Or, at a minimum, the cost of care grows at a slower rate than the historical growth pattern. Organizations may be familiar with total cost of care programs in the form of shared savings programs, which are represented in Level 1 and Level 2 of the NYS Roadmap. Population health management (and true clinical integration) are imperative to success in these programs, as is data transparency and portability.
- Integrated Primary Care (also known as alternative primary care payments or enhanced primary care): These are payment mechanisms tied to the primary care physician (PCP). They consider the PCP’s significant role in the total cost of care for a patient, and also acknowledge the effort and impact of care management by offering a per member/per month (PMPM) for care management.
- Acute and Chronic Bundles (also known simply as bundled payments): These are partial risk arrangements where the services related to an episode (e.g. pre-operative procedures, surgery, recovery, physical therapy and related services and fees) or the management of a chronic condition (e.g. management of a patient with diabetes) are paid to a provider or network of providers and facilities.
- Total Care for a Subpopulation (or “Total Cost of Care” for a subpopulation): These payment mechanisms are much the same as the Total Cost of Care described above, but the population is comprised of members attributed to a subpopulation (a cohort) based on certain criteria. For example, an integrated delivery network may take on management of the total cost of care for a subpopulation of patients with a specific set of co-morbidities or disabilities.
Implementation
What aspects should be considered when contracting for VBP
Integrated delivery networks considering entering into VBP arrangements with MCOs have many considerations for what models would be most appropriate, but must also work with their network participants to understand the evolution that needs to take to achieve their desired state. During the health maintenance organization (HMO) boom of years past, organizations that were not fully integrated found out that bearing risk comes with significant responsibility for care model improvement and constant monitoring.
Strategies for Managing Risk Under VBP
Management of any substantial risk is a complex business. It is common knowledge across the industry that major infrastructure needs be built, optimized and appropriate used to manage risk across the continuum of care. Success in NYS DSRIP is tied to the development of such infrastructure, processes and integration points between clinical care, community based organizations, and other support services to ensure the improvement in outcomes and health status for the Medicaid population. This is the main path to risk management. It is no coincidence that the strategies and tactics for achieving success in various VBP methodologies are very similar:
- It is imperative to interdependence along the continuum of care, both in delivery and follow-up but also in aligned financial incentives and clinical data. NYS DSRIP provides over a billion dollars to be used to drive this work through the PPSs.
- It is prudent to maximize clinical governance involvement in care delivery and administrative support in managing the integrity and availability of data to the network.
- The adoption of evidence-based guidelines for chronic disease management and other tenets of clinical integration programs have been shown to drive success in population health management across disparate populations.
For support in the development of VBP arrangements for your healthcare organization, please contact info@copehealthsolutions.com