


Rural Health Transformation in New York: What Federal Funding Means for Rural Providers, Hospitals, and FQHCs



How CMS is Sequencing Rural Health Transformation for Value-Based Care Success
The next phase of rural health transformation is not being driven by a single payment model, but by the intentional interaction of multiple CMS initiatives, each designed to address a different barrier to value-based care.
On December 29, 2025, the Centers for Medicare & Medicaid Services announced the amounts that all 50 states would receive under the Rural Health Transformation (RHT) Program. This five-year initiative will distribute $50 billion nationally, beginning in 2026, to strengthen and modernize rural health care delivery. New York alone is slated to receive over $212 million in the first year.
At the same time, CMS has introduced new complementary models, most notably ACCESS and LEAD, that reinforce CMS’s commitment to move rural and safety-net providers toward sustainable value-based payment.
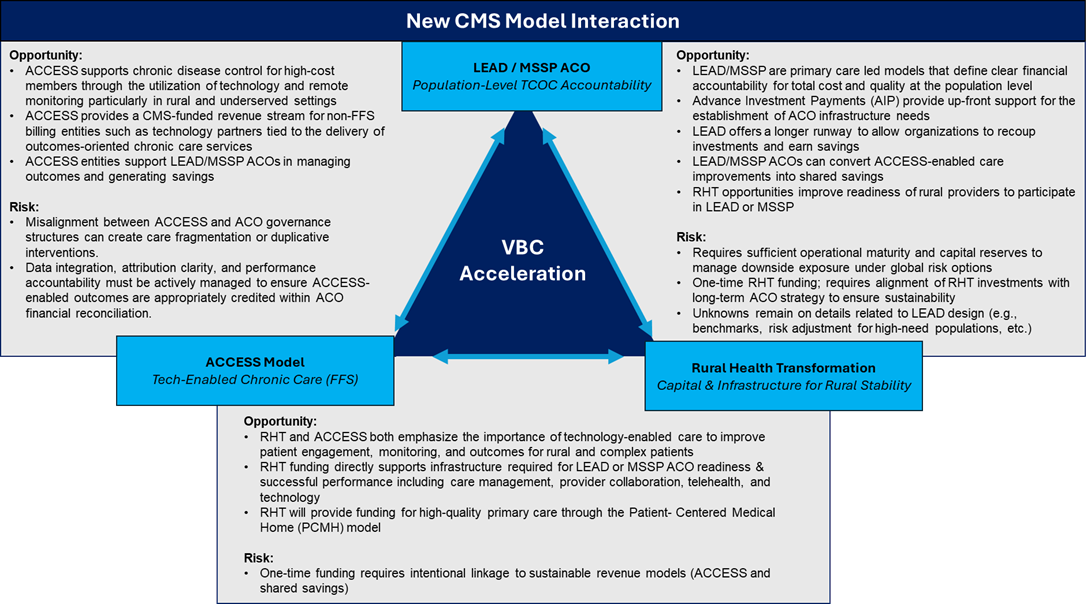
Taken together, RHT, ACCESS, LEAD, and the existing MSSP ACO program with its advanced investment payment (AIP), form a cohesive strategy with a clear and deliberate progression:
Capital & infrastructure → Operational activation → Population-level financial accountability
This sequencing, designed by CMS and reinforced through state strategies like New York’s, creates a powerful VBC acceleration pathway for rural and safety net providers across multiple lines of business, including both Medicaid and Medicare.
- RHT stabilizes the delivery system by providing risk-free capital to strengthen sustainable access, workforce, population health management and technological capabilities
- ACCESS activates a new funding stream for care delivery focused on clinical outcomes, enabling technology-supported care management and partnerships with community providers
- LEAD / MSSP ACO introduces population-level accountability, converting operational performance into shared savings or losses
Together, these programs form a structured on-ramp to sustainable value-based payment in rural markets.
RHT plays a foundational role. New York’s application makes clear that this program is not intended to drive utilization or short-term performance improvement. Instead, RHT provides no cost capital to stabilize vulnerable providers and address long standing gaps in care coordination, workforce capacity, technology infrastructure, cybersecurity, and regional collaboration. These are precisely the elements that fee-for-service reimbursement has historically failed to support, yet they are prerequisites for success under any population based model.
For providers, this distinction matters. RHT funding should not be viewed as a traditional grant, but as pre-paid value-based care infrastructure. Its purpose is to reduce operational fragility and enable population centric delivery models that can later support accountability. An effective RHT investment should measurably reduce future PMPM volatility, improve attribution stability, generate service efficiencies, and decrease fragmentation across the care continuum. If it does not, it is unlikely to be sustainable once the funding period ends.
What does this mean for New York providers?
The opportunity created by the RHT grant is amplified by the state’s ongoing commitment to its Safety Net Transformation Program. Beginning in State Fiscal Year 2025, the Safety Net Transformation program opened funding to support safety-net hospitals in improving access, equity, quality, and financial sustainability through collaborative partnerships. For safety-net facilities serving rural populations, the combination of Safety Net Transformation funding and RHT capital creates a rare opportunity to stabilize finances while simultaneously building the infrastructure required for long-term participation in value-based care.
When layered together, RHT and Safety Net Transformation funding can support workforce investments, technology modernization, and regional integration. Coordinated efforts with ACCESS providers can then be used to operationalize care management and patient engagement. Over time, this combination positions rural Safety Net providers and partnering organizations to participate confidently in LEAD or MSSP ACO and to generate performance-based returns that extend beyond the grant period.
This framework is especially well suited to Federally Qualified Health Centers, which already function as population anchors in many rural communities. New York’s explicit emphasis on the Patient-Centered Medical Home (PCMH) within the RHT program represents a meaningful opportunity for FQHCs serving these members. RHT funding can be used to strengthen and formalize core PCMH capabilities that FQHCs already rely on such as team-based care, care management, care coordination, and continuous quality improvement, without requiring a shift away from their prospective payment structure. By financing the infrastructure and workforce needed to operate at scale as a PCMH, RHT allows FQHCs to stabilize primary care delivery, positioning themselves well for future participation in value-based arrangements, including LEAD or MSSP.
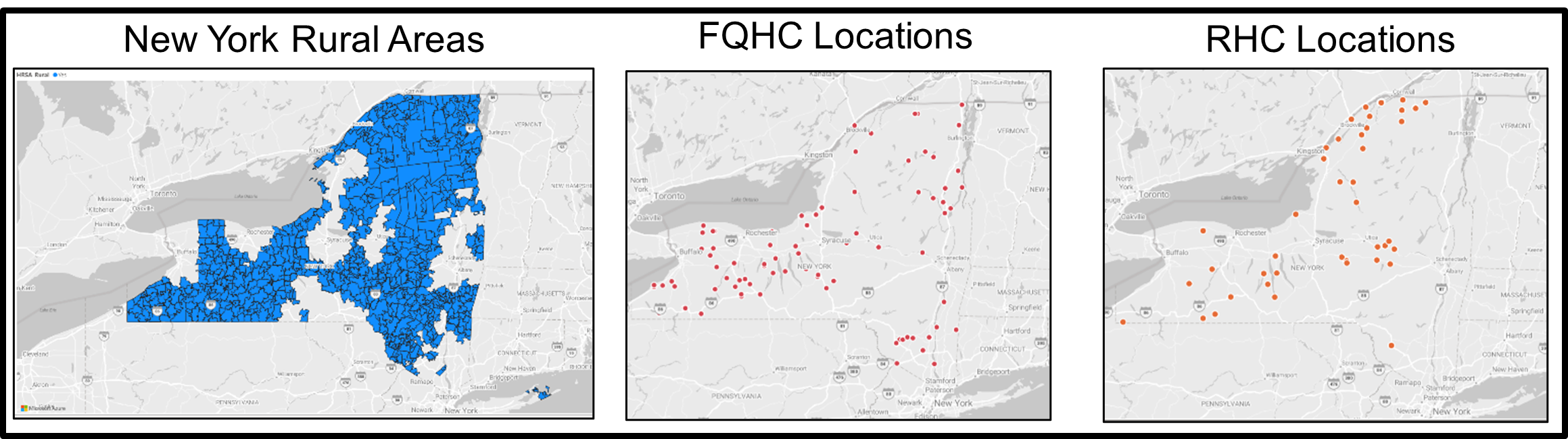
Rural Health Clinics will see more funding opportunities to support infrastructure maturation as well. RHCs benefit more acutely from RHT funding to support care coordination and staffing. RHCs, while often constrained by scale and capital, play an integral role in serving the rural population therefore integrated rural networks will require engagement and co-development with these clinics for success.
Ultimately, New York’s Rural Health Transformation Plan is about alignment. Providers that understand how RHT, ACCESS, and LEAD/MSSP ACO reinforce one another across both Medicaid and Medicare fee-for-service populations can turn geography into strategy, infrastructure into leverage, and population focus into sustainable value-based success. Those that pursue these programs in isolation risk achieving short-term gains without long-term impact.
More information regarding the ACCESS Model and Lead Programs can be found in our federal healthcare policy update.
How to Prepare
Now is the time for providers to take deliberate steps that will position themselves for long term success, ahead of the state’s official notice of funding opportunities. Organizations and providers alike should begin to:
- Assess their readiness, including data infrastructure, quality reporting capabilities, and population health management capacity.
- Understand the efficiency weaknesses of operational & management services that may impact performance as a network partner such as financial systems, coding and rev cycle
- Strengthen regional partnerships across hospitals, FQHCs, clinics, behavioural health providers, SCNs and community partners to support coordinated, ecosystem level strategies.
- Align with Medicaid financing and other grant funding (i.e. Safety Net Transformation Program) to ensure RHT initiatives complement existing funding
- Plan for accountability and sustainability, with a focus on measurable outcomes, operational efficiency, and reinvestment beyond the funding period.
COPE Health Solutions supports stakeholders across all four areas through a combination of strategic consulting services and its ARC Population Health Management Platform. Our expertise helps rural providers evaluate readiness, align regional strategies, operationalize performance measurement, and build sustainable care models that are positioned for success within this state specific and other federal initiatives.
For more information and to talk through your organization’s next move, reach out to us at info@copehealthsolutions.com or visit us at copehealthsolutions.com.