4 Things for Washington Providers to Know About the CMS MCP Request for Application






![]()
On August 14, CMS published the Request For Application (RFA) for Making Care Primary (MCP), a progressive roadmap to value-based payment for primary care providers with little-to-no VBP experience. CMS has indicated that the program may be aligned with the upcoming Washington 1115 Medicaid Waiver amendment which will have its own primary care enhancement program for Medicaid. Therefore, there are opportunities for MCP participants in Washington to leverage both programs to optimize financial and clinical outcomes.
MCP’s payment, quality and care delivery designs are meant to enhance primary care setting population health management capabilities and build off prior advanced primary care models, such as Primary Care First (PCF) and Comprehensive Primary Care Plus (CPC). What’s new in this model are the health equity and state Medicaid alignment initiatives, which could be highly beneficial depending on the final details of the Washington 1115 Medicaid Waiver Amendment.
The model is a good fit for primary care providers, including federally qualified health centers (FQHCs), with limited care management and health IT capabilities or limited experience operating in a value-based environment and closing health-related social needs (HRSN) gaps. The investments made available to MCP participants and the upside-only nature of the program would help MCP participants both build out the capabilities and gain the experience needed to succeed in riskier VBP arrangements. ACO Reach participants are ineligible for MCP, and providers must be out of the Medicare Shared Savings Program (MSSP) by 12/31/24 to be eligible for MCP. CHS can support interested parties who have applied or plan to apply to MCP analyze which model would best serve their financial and operational interests in the immediate and longer-term future.
Here are 5 key considerations that MCP applicants should be aware of:
1. CMS will provide investments in Track 1 and increase performance incentives in Tracks 2 & 3:
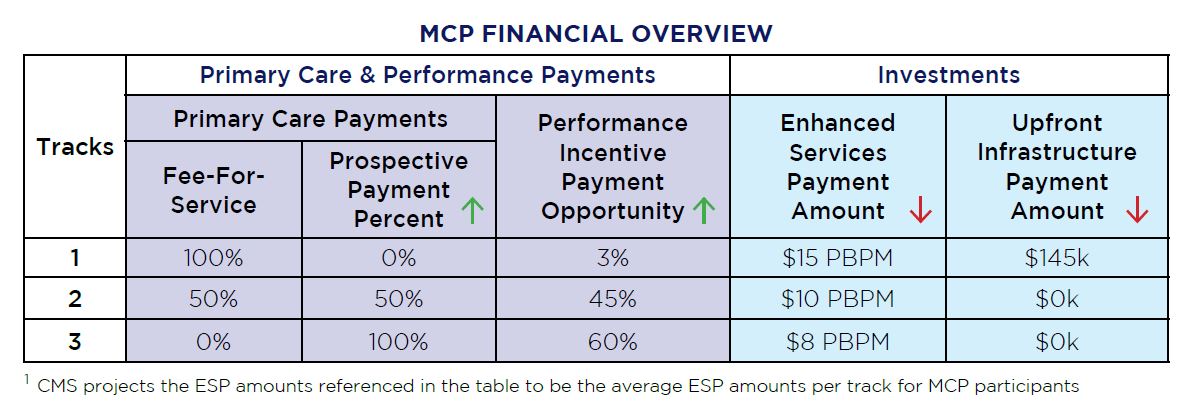
- Primary Care & Performance Payments:
- Primary Care Payment percentages reflect the proportion of fee-for-service (FFS) vs Prospective Primary Care Payments (PPCP) payments an MCP participant will receive in primary care service reimbursement on by track
- Performance Incentive Payment (PIP) percentages reflect the proportion of primary care payments eligible for bonus
- The actual bonus amount earned by an MCP participant will be contingent on performance against quality measures
- CHS can help MCP participants maximize their PIP by providing the care management and data analytics support needed to close care gaps and achieve quality measures
- Investments:
-
- Enhanced Services Payments (ESP) are clinically and socially risk-adjusted care management fees paid on a quarterly prospective basis ranging from $2-$25 PBPM to support enhanced Care Management activities
- Actual ESP payment amounts will be impacted by MCP attributed beneficiary’s low-income status (LIS) and clinical and social risk adjustment factors
- The maximum ESP amount eligible for a beneficiary is $25 PBPM
- ESP payments will decrease by 50% track-over-track
- CHS can help your organization build out the coding practices needed to maximize your ESP amount
- Upfront Infrastructure Payments (UIP) are only available to MCP participants in Track 1 that meet eligibility requirements below:
- Meets the “low-revenue” threshold: Part A +B revenue/spend < 35%
- Does not have an e-consult platform
- Enhanced Services Payments (ESP) are clinically and socially risk-adjusted care management fees paid on a quarterly prospective basis ranging from $2-$25 PBPM to support enhanced Care Management activities
-
The graph below illustrates a CMS projection of MCP payments provided in a MCP webinar. CMS has also published an Example Revenues Fact Sheet here.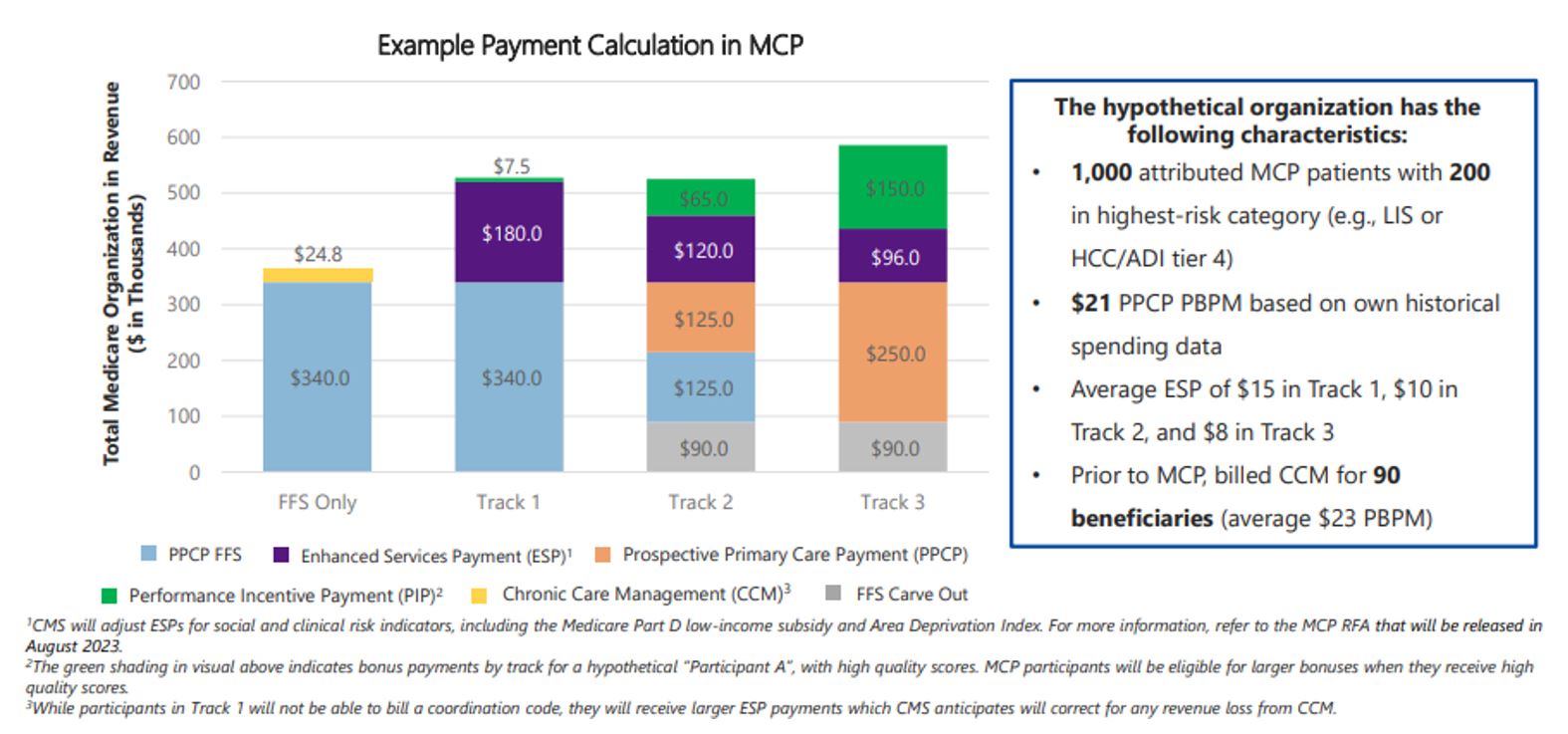
2. CMS is using a design-implement-optimize care delivery build roadmap for MCP participants to follow:
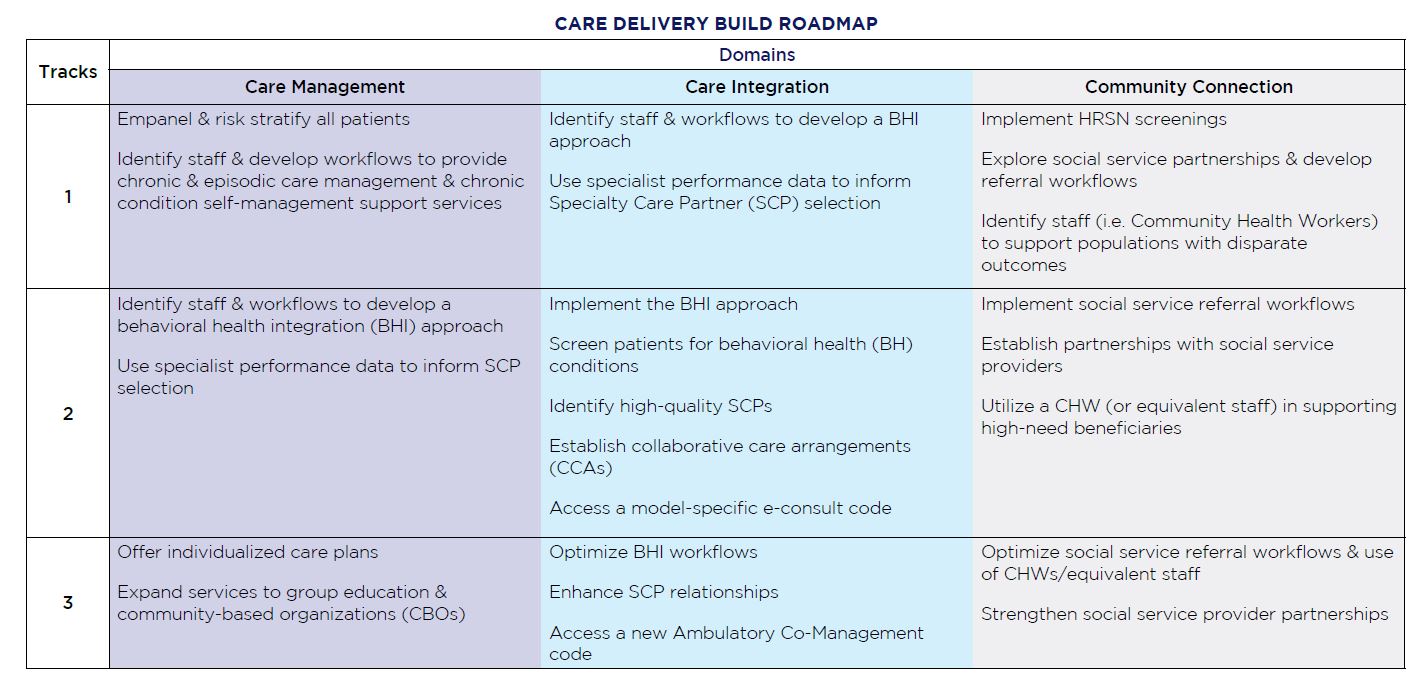
CHS can support MCP Participants through each phase of the Care Delivery domain roadmap through care model best practices, healthcare workforce and data analytics support across clinical and social services workflows.
3. CMS will implement Health Equity requirements similar to those in ACO REACH:
- MCP HEPs to identify patient outcome disparities, implement initiatives that measure and reduce disparities over the course of the model, and submit annual HEP update reports
- CMS will provide an HEP template to MCP Participants
- MCP participants must submit beneficiary-level demographic data for MCP attributed patients and aggregate-level HRSN data for all patients
- CHS can support MCP participants through the submission and implementation of Health Equity Plans and the infrastructure build needed to capture demographic and HRSN data efficiently
4. CMS will provide data and partner with State Medicaid agencies to support MCP participants:
- CMS will provide quality, utilization and payment metrics, attribution reports and data from multiple payers through state-based resources
- MCP participants can compare their metrics to other model participants and obtain specialist data to inform Specialty Care Partner selection
- CMS will provide learning opportunities to MCP participants through platforms and partnerships
- CMS will provide a collaboration and care delivery platform on which MCP participants can learn from each other and share tools and resources
- CMS will work with state Medicaid agencies and other payer partners to connect MCP participants with CBO connections, practice coaching and data aggregation resources
- CMS will partner with State Medicaid agencies and encourage payer partnership to align key MCP program components with other primary care programs across LOBs
If you are interested in learning more about steps after applying to MCP, please reach out to Adam Lipton (alipton@s4ch.net.org), Allison Bergmann (abergmann@s4ch.net) or email info@copehealthsolutions.com to learn how CHS can help your organization succeed in MCP or any other form of value based payment for Medicare, Medicaid or commercial lines of business.
To learn more about how S4CH can help your FQHC or other health organization succeed through state-of-the-art strategic advisory, patient experience, and technology analytics supports, visit S4CH or call 1-866-519-7424.
Call 213-259-0245 to learn more about how CHS can help your organization to succeed in this CMMI model or any other form of value based payment for Medicare, Medicaid or commercial lines of business.